

Here’s my trail of questions and findings..
I set up a community farm called Lovebrook here in Sussex in the UK. On Fridays I lead a community health session. I’m not medically trained but that doesn’t matter. The idea is that we tap into the deep pool of health knowledge and experience that the community already has. We share what we know on a topic, support each other, work on the farm, and then share a wholesome lunch.
This question came up: ‘I know viruses exist, but how do we know that they exist?’. None of us had the answer, so I thought I should do the question justice and go away and try to answer it as well as I could. I thought I’d probably be able to find a good lab image of a virus and come back to the group to explain the process of how the virologist isolated and identified it.
To my surprise, it didn’t quite turn out like that. Here’s what I found.
1. What are the techniques that virologists use to identify viruses?
I discovered a whole toolbox of methods that are used in virology — including filtration, cell culture effects, imaging, molecular detection, immune assays, animal studies, and metagenomics.
What surprised me was that all these different techniques already assume the existence of a virus. They don’t really test whether a virus exists — they start from that idea and then build everything on top of it
While these techniques differ technically, their results are interpreted within a framework that presupposes viruses – using techniques that rely on software models built from assumed viral genomes, or automatically interpreting toxicity and cell damage as biological invasion.
I found this confusing because I didn’t understand how this could be squared with the scientific method. If none of these methods can directly show that a virus exists, how can hypotheses about viruses be tested?
This was not a good start.
So I decided to find out more about one major technique – CPE
2. How does CPE provide evidence?
I found out that CPE is the routine way to demonstrate the pathological properties of viruses in the lab. The technique is to add suspect virus samples to cells in culture. When the cells begin to die, we have the so-called “cytopathic effect” or CPE.
However, I found out that this technique was not what it seemed.
According to Dr Mike Yeadon a Biopharma research scientist and former Vice President at Pfizer, what he discovered about CPE was:
“so unbelievable that I rejected it for over two years after I was told about it. Cells die not because a clinical sample, thought to contain a virus was added, but because the researchers, following a 70-year-old recipe, radically reduce the growth factors necessary to keep the cells alive and add high concentrations of antibiotics (ostensibly to retain bacterial sterility).”
He goes on: “You may be thinking ‘This cannot be right because, if it was, the control leg of such a study would report CPE even with no supposed pathogen’. Here’s the shock. None of the papers reporting, for example, “The isolation of SARS-CoV-2” ever include these controls. What this means is that, uniquely in virology, the scientific editors & peer reviewers have become accustomed to not expecting to see control legs and results.”
3. So we just need to do the proper control studies then?
I discovered that over the past two years, Jamie Andrews, Albert Mathews and a team of microbiologists and Geneticists at the Virology Control Study Project, has gone back to the root of this central method in virology and, using contract research organisations, performed the necessary control studies. In every case, when they looked at the cells after growth factor dilution and addition of antibiotics, they see the cells begin to die off, that is, CPE occurs. They have repeatedly confirmed that it’s the protocol & not the purported “virus” which causes cells to die.
What this suggests is that the most important technique for “confirming the cytotoxic effect of viruses” has been carried out without controls since the first time it was reported on in the 1950s, (when it turns out a Nobel Prize was awarded).
4. Ok, regardless of whether we can confirm the effects of viruses, I’m sure I’ve seen actual images of them?
I initially looked into the technique regarded as the most advanced for visualising viruses – ‘cryo-electron microscopy’ (cyro-EM). This method freezes samples to produce high-resolution images of so-called purified ‘virions’ (viruses outside of the cell). However, as I looked more closely, I found that purification and identification elements of this technique relied on prior selection, and agreement with genomic and immunological models – meaning the images only make sense once those assumptions are already in place.
The images of viruses that I have seen in the media would have been captured not through cyro-EM but through general electron microscopy (EM). This is the principal method used to visualise viruses at high resolution. However this method is also not as simple as I thought. It requires cells or cell lines to be removed from their living context and subjected to extensive artificial preparation—including chemical fixation, dehydration, heavy-metal staining, sectioning, and vacuum exposure—meaning the resulting images depict static, highly processed specimens rather than intact, living biological systems.
I learned that the images we see in textbooks are cleaned up high contrast images, and what microscopists actually have to work with is a soup of variegated cell material. Areas of interest can be magnified to find particles that correspond to the size and shape of known viruses, and then this data is triangulated using other (model based) identification techniques.
Viruses where viruses shouldn’t exist
Intriguingly though, researchers such as Dr Stephan Lanka claim that they have identified structures with all the requisite size, morphology and location patterns of a bona fide virus, but in places where viruses definitely shouldn’t exist.
In 2025 The Virus Control Studies Project (VCSP) provided confirmation of this. They sent verified virus-free cell lines with all the requisite contamination controls to reputable labs and contracted them to explore the cell lines to identify potential viruses. The labs were blind to the rationale for this routine investigation.

The Virology Controls Study Project
The results were striking. VCSP videos of these microscopy sessions were comprehensively and methodically recorded, video-recorded and published. They show that examples of many families of viruses were found by microscopists – oval shaped retroviruses, corona enveloped viruses, icosahedral herpes viruses, large ovoid pox viruses and even evidence of viral ‘budding’ and other phenomena you would expect to see in contaminated cell lines – all within a verified virus free cell line.
The obvious question here is if these are not viruses, what are microscopists seeing?
The researchers suggest that they can only be looking at dead and dying cellular debris — vesicles, blebs, and fragments produced during cell injury and death. I discovered that microscopists say they routinely see ‘lookalikes’, but if VCSP’s research is correct (and this is relatively cheap to independently replicate and very easy for any curious virologist to confirm), this suggests that everything could just be a ‘lookalike’.
This is an extraordinary situation. If confirmed it would mean that for decades technicians have been expecting to see ‘known’ viruses and then doing nothing more than the equivalent of finding faces in clouds.
5. What about images of viruses in the blood?
I now knew that if I was going to find the solid evidence I was looking for, It would probably have to come from a process that avoided all the artificial preparation and complexities of electron microscopy and CPE. I decided to find out what could be seen in the blood. I knew that Pox viruses were said to be blood borne, and I knew that it was possible to capture images of small structures in the blood because I had seen images of them.
The microscope technique used here is called light microscopy which is a much more direct process than electron microscopy. I found out that all sorts of structures inside cells in the blood such as mitochondria, and granules are directly visible through this apparatus – which was very promising since Pox viruses are the same size as these already seen structures at 200 – 300 nm.
Frustratingly however, these viruses are said to remain invisible to light microscopy not because of their size, but because they are said to be transient and lack contrast. Because of this, light microscopy wouldn’t be expected to see them.
6. Ok, so even if there are problems with lab techniques, there must be lots of experiments proving contagion?
I felt I was sure to find good evidence here, particularly with colds and flu being so common. However, again I came up against extraordinary claims such as this by Dr Tom Cowan in his book ‘The Contagion Myth’ co-authored by Sally Fallon Morell: ‘You will not find a single paper that directly proves natural human-to-human transmission of a virus’. This sounded like the gauntlet was being thrown down here so I explored further. I then discovered that in the UK The Common Cold Unit in Salisbury produced 40 years worth of data that failed to demonstrate natural human contagion.
Mike Yeadon has discovered the same phenomenon. After a career specialising in respiratory diseases he created a Substack repository of every published study on attempted transmission of colds and flu. These papers start in 1918 & continue until 2024. He claims that in not a single paper do healthy volunteers develop symptoms, after spending time with a symptomatic person, any more often than when the volunteers spent the same amount of time with a well person – suggesting that respiratory illnesses do not seem to be contagious.
Animal experiments
Even animal contagion experiments appear to be unsatisfactory. As Dr Andrew Kaufman has pointed out, even the most frequently cited animal “contagion” experiments typically involve injections of ground tissue, force-feeding of pathological material, and conditions of extreme confinement, stress, or deprivation – perhaps less proof of contagion, and more proof that you can make an animal sick by poisoning or injuring it.
Contagion papers
If contagion is being asserted, then it seems obvious that I should be looking for evidence that shows natural transmission under ordinary, non-coercive conditions. When I drilled down into specific papers the human transmission studies topic became even more intriguing. For example:
HIV: In the longitudinal study by Padian and Padian researchers followed sexually active couples, where one partner was HIV-positive and the other HIV-negative, but under the conditions of this study found no documented cases of HIV transmission between partners.
SARS-CoV-2: In one of the most widely discussed human challenge studies of COVID-19 at Imperial College London, healthy volunteers were deliberately exposed to SARS-CoV-2. Most developed either no symptoms or only mild rhinitis symptoms. Some commentators have noted that participants underwent frequent nasal sampling. Though not identified as a causal factor in the study itself, they speculate that this was the cause of the observed rhinitis.
INFLUENZA: In a 2020 human challenge-transmission study led by Jonathan S. Nguyen-Van-Tam and colleagues, healthy volunteers infected with influenza A (H3N2) were exposed to other participants in a controlled setting, but there was ‘minimal’ evidence of transmission under those conditions (1 in 75 participants).
In a subsequent follow-up human challenge study published in 2026 by Jainyu Lai and other notable virologists and epidemiologists, it was reported that ‘no recipient developed influenza-like illness, PCR-positive respiratory samples, or serological evidence of infection following controlled exposure to infected donors.’
This theme is echoed throughout Daniel Roytas’ book ‘Can you catch a cold?’ (2024). He reveals that he spent years searching for all the studies he could find on human to human transmission of viruses. It turned out that none of the more than 200 studies that he found showed transmission.
7. But I have seen evidence of contagion with my own eyes!
Like everyone else It feels obvious to me that we “catch colds” from other people. I’ve noticed the sequencing of illnesses happen in ways that are consistent with contagion. However if I really have to think about it, that’s all it is, consistent with contagion but not proof of it.
So in the spirit of the question ‘how do we know that viruses exist?’ I realise that while I’ve witnessed what looks like contagion in my household, I know that I also routinely witness close contact resulting in no transmission. Similarly, I have come across anecdotes from doctors and health workers reporting that they spent whole careers working with infectious disease patients while also remaining mysteriously ‘immune’.
Patterns from events
I noticed that I form patterns from events. When I develop a cold, I remember recent contact with someone who had a cold, but I never consider that contact if it didn’t lead to me catching a cold. My expectations seem to be central to this too. For example I’d never find myself wondering who I might have caught a headache from as I already know that headaches are not contagious.
So although I may think I am observing patterns of disease due to pathogenic contagion, in reality I can’t rely on this as evidence of contagion.
8. So what is making us sick then? If there’s no good alternative theory for colds and flu then it must be a virus, right?
The virus explanation has framed my understanding of sickness for as long as I can remember, so removing it to consider an alternative felt a bit like like stepping into conceptual thin air at first. This is where I learned about ‘Terrain theory’ as an alternative to ‘Germ theory’. This holds that people become ill because their internal environment is compromised, not because they are attacked by external pathogens. In terms of specific alternative causes for viral disease, like most people I was under the impression that there weren’t any. However it turns out that there is actually no end to the list of proposed non-virus causes, eg:
Toxic exposures (chemicals, pesticides, pollution, pharmaceuticals), Nutrition, Poor diet (ultra-processed foods, seed oils, sugar, alcohol), Dehydration, Chronic stress, Emotional shock, Unresolved trauma, Poor sleep, Lack of sunlight and fresh air, Poor gut function, Accumulated cellular waste, Metabolic stress, Poor circulation, Mold and biotoxins, Physical injury, Early years separation anxiety, Medical interventions, Psychological conflict, Fear, Noise, EMFs, Radiation, Temperature extremes, Social stress, Loneliness, the list goes on..
Flu
Just to give one example, here’s an explanation put forward which sounds quite plausible to my (non-medically trained) mind:
Dr Ray Peat describes colds and flu-like illnesses as ‘states of metabolic stress in which temperature regulation, cellular respiration, and tissue renewal are impaired. Seasonal cold, reduced light, and stress hormones compromise the body’s ability to maintain healthy mucosal tissues, leading to inflammation, mucus production, and fatigue until normal metabolic balance is restored.’
Terrain or immunity?
And isn’t mainstream medicine an advocate of terrain theory anyway? Isn’t ‘metabolic stress’ or ‘loss of equilibrium’ basically the same as the mainstream idea of ‘low immunity’? What I find interesting here is that where mainstream medicine says disease strikes the weak, terrain theory seems to be asking why people become weak, and as modern medicine increasingly focuses on stress, toxicity, nutrition, and resilience, it seems to be drifting ever closer to terrain theory—while still speaking the language of pathogens and immunity.
9. Is there any evidence from ancient health systems? Did they notice contagion?
It seems that over three thousand years of Ayurvedic and Chinese medicine practice, doctors didn’t notice the contagion that we now take for granted.
-
Records show that respiratory illnesses we now label as colds, flu, or COVID-like syndromes were attributed to seasonal influences — such as cold, damp, wind, and reduced sunlight — acting on a vulnerable terrain. When multiple members of a household became ill, this clustering was explained through shared living conditions: the same air, the same food, the same routines, and the same environmental stresses, rather than through the transmission of a specific infectious agent.
-
These traditions also recognised clusters of distinct childhood illnesses — what we now call measles, mumps, or chickenpox — but understood them as collective or seasonal imbalances affecting communities, sometimes described as environmental or “toxic” influences.
-
Conditions we would now classify as gastrointestinal viral infections were largely attributed to contaminated food or water, impaired digestion, and weakened bodily resilience.
-
Sexually transmitted illnesses, by contrast, were well recognised as arising through intimate bodily contact and exchange of fluids — indicating that while contact-based illness was clearly observed, it was not framed through the modern concept of invisible, replicating microbes.
Contact yes, contagion no.
It was at this point that I understood an important distinction. While the idea of invisible, invading pathogens that spread from person to person is a relatively recent development, humans have always recognised that people can influence one another’s biology through close contact. Sexual contact is an obvious example, but not the only one.
In fact, we continue to recognise this today. There is a growing appreciation of non-viral ways in which biology can be shared or influenced — through bodily fluids, bacteria, signalling molecules, stress chemistry, and other forms of physiological coupling. These influences can shape health without requiring the transmission of a discrete infectious agent.
These ancient medical systems appear to have taken these shared biological influences for granted. They presupposed phenomena that modern science still struggles to explain mechanistically, such as the synchronisation of menstrual cycles among women living together. These traditions did not deny interaction between bodies. They understood it in systemic and relational terms rather than through the modern lens of microbial invasion.
Pre-scientific
So it seems ancient health systems didn’t have a concept of invisible, replicating viruses. Previously, I might have interpreted this as evidence that they were pre-scientific, intellectually primitive, or simply lacking modern tools. Now I’m not so sure.
10. But how do we explain all that historic evidence of vaccines spectacularly stopping epidemic viral diseases in their tracks?
What I found on this topic was a big surprise too. In their book ‘Dissolving Illusions’ Suzanne Humphries MD and Roman Bystrianyk used official government data to reveal historic mortality rates from infectious diseases.
I expected to see graphs here showing a century of devastating diseases being halted by the introduction of vaccines. What I found was mortality rates of scarlet fever, whooping cough, measles, diphtheria and smallpox continuing on their downward track and close to 0% by the time vaccines were introduced. The authors explain how improvements in living conditions, sanitation, nutrition, and the abandonment of harmful medical practices led to the decline of these diseases and how the medical profession has systematically misinterpreted and ignored key historical information.
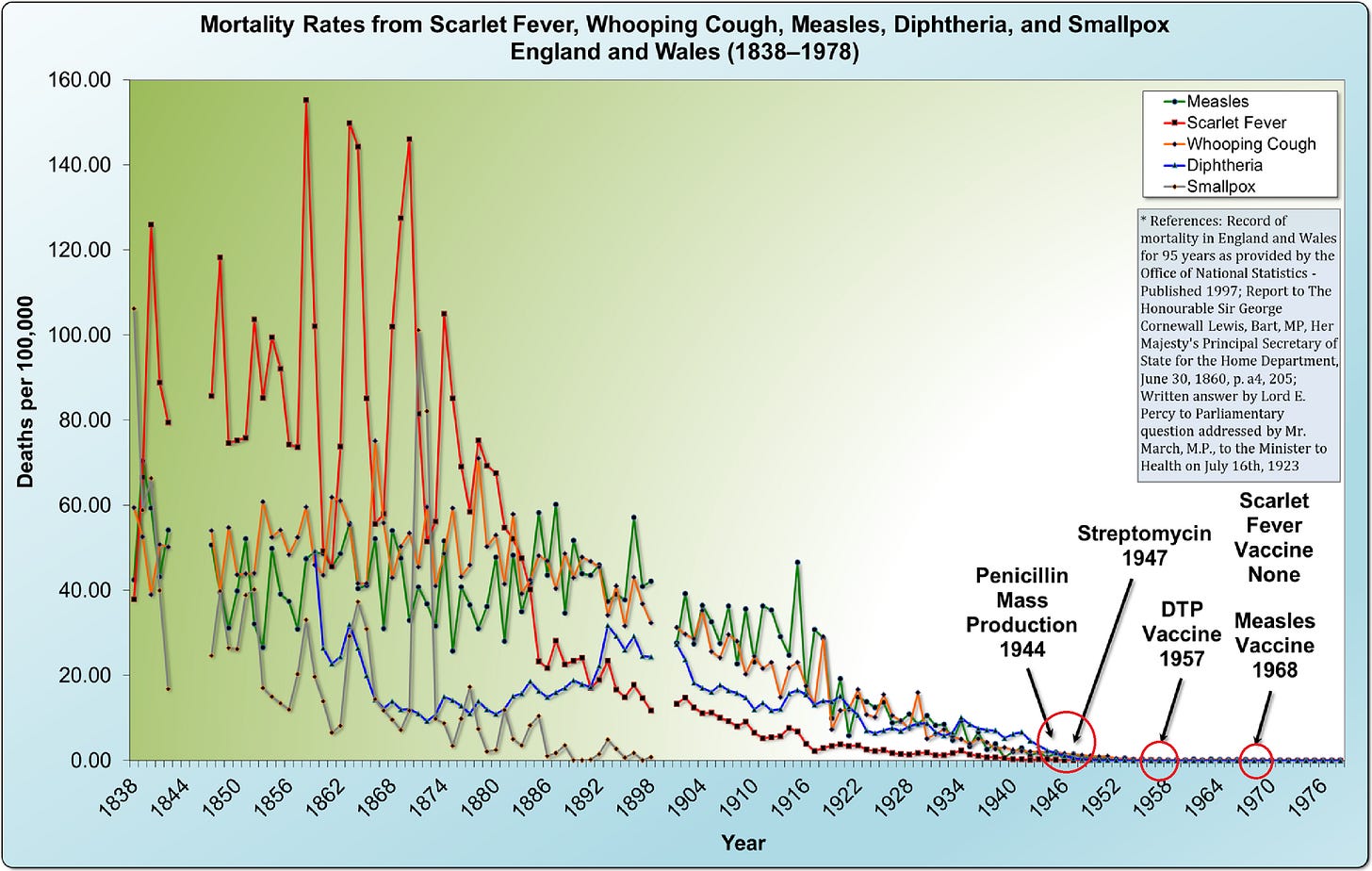
‘Dissolving Illusions’ Suzanne Humphries MD and Roman Bystrianyk
So it seems clear from this graph alone that I was not going to be able to use the historic efficacy of vaccines as my evidence for the existence of viruses.
11. What about PCR testing – isn’t this used across-the-board to detect viruses?
Again, it seems that as soon as I scratched the surface, this is another topic that seems to be far from settled. This is what I found out:
-
PCR works by amplifying tiny amounts of specific DNA or RNA sequences into millions or billions of copies so they can be detected and measured
-
It can’t detect a virus as an entity
-
It can’t demonstrate replication, infectivity, transmission, or causation
-
What is often called “viral load” can be understood as a laboratory construct — a signal reflecting biochemical activity detected by PCR. It is interpreted as evidence of viral replication only because virology assumes viruses exist. If that assumption is set aside, the same signal could equally be read as a non-specific marker of physiological disturbance
-
A peer reviewed paper by Günther, Rockenfeller & Walach, published in Frontiers in Epidemiology (2025) shows how often a positive PCR test actually matches up with real biological infection as measured by serology. Astonishingly, their finding was just 14% of the time.
It seems that before PCR even starts, the “virus” already exists as a theoretical genetic construct. And if we conclude from the Günther 2025 paper that PCR tests can’t be trusted, this raises huge questions for all those asymptomatic people for whom PCR has confirmed that they are living with a viral disease. I discovered for example that PCR is still routinely used for infant HIV diagnosis.
What does PCR detect then?
Before I moved on from exploring PCR I was left with the obvious question of ‘what is PCR detecting if it is not viral genetic material?’ Terrain theory adherents point out that the body does produce particles as part of detoxification and repair, which could be detected by PCR, and speculate that the answer could be that PCR is detecting ‘charge’. It may well be responding to the presence of charged molecular fragments produced by cellular breakdown or biochemical disturbance, rather than detecting a specific living infectious agent.
12. What about deadly pandemics such as Spanish Flu?
This is often described as the most deadly pandemic in history. I discovered that it had novel features, it targetted healthy young men, it was highly contagious, and it was said to quickly spread across the world.
During the pandemic in 1918 – 1919 the US health service undertook a major experiment to directly prove person-to-person contagion under controlled conditions.
According to Sally Fallon, president of Weston A. Price Foundation:
-
The Rosenau experiment used 100 navy volunteers with no history of influenza.
-
They were made to breathe sick patient’s air, have coughing into their faces, share saliva, and had material from sick people injected into their noses and throats.
-
Not one volunteer developed flu
Spanish flu in context
A documentary by Drs Mark and Sam Bailey suggests that we must put the Rosenau results in context:
Epidemics have always appeared where biologic systems are weakened. A lack of food and water, poor sanitation, toxic overload, intense social stressors – these things define the world of 1918 and the social conditions of the great war.
As to why the victims were healthy adults and not the old and very young? They point to soldiers being exposed to three years of chemical warfare, with thousands of tons of chemicals put into the air across a continent. They also site poor nutrition and living conditions and point to the historical accounts that document the crude mass injection of several million people with experimental bacterial vaccines at the time. They question who the Spanish Flu virus narrative served at the time, and note that the Spanish Flu disappeared at the end of the war.
When I looked beyond the usual narrative, rather than finding the virus evidence I was looking for, all I found was more doubts and questions regarding Spanish flu.

The Rosenau Experiement
13. And the AIDS pandemic, how do we make sense of that?
This is an epidemic that formed the backdrop to my early twenties and I remember how it dominated global culture at the time. To question it feels like heresy. According to Dr Eleni Papadopulos-Eleopulos and others in the grouping known as The Perth School though, the HIV/AIDS narrative became institutionalised before being fully proven. They point out that dissenting scientists were marginalised rather than debated.
The HIV Control Studies Project – a community of individuals diagnosed with HIV, continue to point out that Luc Montagnier and Robert Gallo, the discoverers of the virus, left significant gaps in their evidence for the virus:
-
They relied on the identification of reverse transcriptase as a specific marker – a marker which turned out to be not specific to retroviruses.
-
The core evidence of purification of the virus could not be shown.
-
Evidence of the ‘knobs’ – essential to the transmission binding function were not shown.
House of numbers
As I delved further I discovered that the epidemic was perhaps not what it seemed. I came across the illuminating documentary ‘House of Numbers: Anatomy of an Epidemic’ (2009) which cast more doubt over the veracity of the pandemic. It showed how the disease showed up in completely different ways in different parts of the world.
The film shows how in the West, AIDS looked like a rare immune-collapse syndrome, and claims some symptoms are consistent with the recreational use of chemical ‘poppers’. In Africa, AIDS looked like extreme poverty and chronic inflammation. The same label was applied to very different clinical pictures. The list of symptoms became very long, and testing and diagnosis was rolled out on a massive scale.
The film also showed how testing was indirect and open to misinterpretation, and asymptomatic people were routinely presented with a ‘death sentence’ diagnosis and offered ‘life-saving’ drugs. The film also presents evidence suggesting that HIV drugs, particularly AZT, were prescribed at highly toxic levels and may have caused symptoms attributed to AIDS, and in some cases caused death.
Model entrenchment
I discovered that there is a growing understanding out there that although a syndrome we call AIDS exists, it has shifting symptom lists over time and geography. The symptoms and suffering may be caused by non-HIV factors such as oxidative damage, toxic drugs, lifestyle factors, malnutrition, and cellular stress.
Again, I was left with more questions than answers here. I found that HIV is frequently held up as meeting modern criteria of causal proof better than any other virus. But if those criteria were developed in the context of HIV research, is this independent confirmation or has virology built itself a self-reinforcing explanatory framework here? Is this just virology’s most sophisticated example of model entrenchment?
14. But ‘antiviral’ drugs seem to work don’t they? Doesn’t this point to the existence of viruses?
From what I could discover, antiviral drugs clearly alter disease courses and laboratory measurements, and many doctors report positive outcomes when prescribing them. The question seems to be not whether the drugs are doing something — they obviously are — but whether their effects require the presence of a pathogenic virus. To get to the root of this question I had to break this down into some sub-questions:
Do predictable drug effects imply a specific viral target?
I discovered that the fact that drugs produce predictable effects doesn’t necessarily mean they’re acting on a virus. These drugs interfere with basic processes inside our own cells — things like how genetic material is copied, how enzymes work, and how cells manage stress.
Doesn’t drug “resistance” reflect viral evolution?
I found out that what looks like “resistance” may simply reflect survivorship — cells that couldn’t tolerate the drug died, while those that adapted survived. Observing what remains after treatment doesn’t necessarily mean a virus evolved; it may mean the system adapted.
Don’t the genetic changes observed after treatment belong to a virus?
Genetic changes detected after treatment may reflect host cellular responses to chemical stress. Sequencing shows what is present after intervention, but interpretation determines whether that signal is called “viral.”
Isn’t the virus model proven to be really good at predicting outbreaks and mutations?
Researchers argue that predictions may be tracking host responses, not pathogens. They argue that seasonal illness, immune signalling, inflammation, metabolic stress, and detoxification responses all follow predictable patterns without requiring a virus.
I found out something else interesting here too. It seems that history is full of scientific models that were predictive and practically useful, yet later shown to be false — from Ptolemaic astronomy to phlogiston. Models can predict without being literally true. Once a viral model is assumed: surveillance looks for viral markers, tests are tuned to those markers, interventions shape outcomes, outcomes validate the model.
Pain particles
So I was left concluding that yes, drugs alter disease outcomes, and doctors see improvements in their patients with antivirals, but this doesn’t prove a virus any more than anaesthesia proves the existence of pain particles. It proves that chemistry can change physiology. The viral explanation remains an interpretation layered onto those effects, not a demonstrated biological fact.
15. Just a hypothesis? How how does virology accommodate all these contradictions and still make the model work?
If you have read this far you’ll know that even though I have explored every line of enquiry I could think of, evidence for the existence of viruses has remained surprisingly elusive. At this point I had allowed myself to contemplate the shocking idea that maybe viruses don’t exist, and therefore what we were dealing with here is a sophisticated multi-layered model.
But I wondered, how does virology accommodate all the contradictions, gaps, and data points that I have set out above? How does it make the model work?
This is where I had to take some time to delve into the history of virology and then try to get a clear understanding of the current lines of reasoning put forward by virologists.
They have to relax Koch’s postulates
In the 19th Century medicine was perceived to be full of associations, anecdotes, circular reasoning and speculation. As a response Robert Koch formulated postulates that became the gold standard for proving disease causation. The postulates boiled down to this:
If something really causes a disease, you should be able to find it, isolate it, make it cause the disease, and find it again.
Although this seems to be a logical approach to moving science forward, I discovered that modern virology moved away from Koch’s original rules. We were invited instead to trust the hypothesis that viruses are not the kind of entities that can be seen directly. So the old rules were relaxed and viruses were no longer required to be isolated as independent organisms. Nor were they required to be shown to directly cause disease in healthy hosts. Instead, because of the proposed nature of viruses, it was accepted that viral causation can only be inferred.
But virologists claim that this is not a weakness. They claim that this is okay because when many different kinds of this inferred evidence are shown to point to the same conclusion, this counts as established evidence that a virus exists and causes disease. This is the main claim of virology.
They claim convergence of inferred evidence is proof
As I have said, I don’t have a scientific background, but something about this line of reasoning just doesn’t add up. If every test is built on the assumption that viruses exist, then agreement between those tests doesn’t prove anything new. Surely agreement between those tests just shows that the same idea is being read back out of different experiments. So virology hasn’t demonstrated a virus as a real, independent cause of disease — it has built a coherent story around that assumption and then treated the coherence as proof.
It‘s as if we are drawing a map first, then pointing to how well all the landmarks line up and claiming that proves the map is the territory.
They defend the idea that ‘inferred proof is enough’ in court
At this point in my journey I had already come across biologist Dr Stefan Lanka.
I discovered that in 2016 Dr Lanka had offered a 100k Euro challenge: ‘show me clear scientific proof of the measles virus and its diameter according to basic scientific standards’. The case ended up in the High Court in Germany in 2016. Dr Lanka was looking for a single paper. A German doctor submitted six scientific publications that together, he argued, demonstrated the existence of the measles virus.
This response is exactly what Dr Lanka was trying to flush out through his challenge and subsequent court case. As expected, virologists claimed that a single piece of direct foundational evidence is too much to ask from modern virology, and papers that show a convergence of inferred evidence is enough.
What Dr Lanka wanted to make transparent here is that if something can only be inferred, never directly demonstrated, and only makes sense inside its own framework, then it should be called a hypothesis — not an established fact. Because the challenge stipulated just one paper, Dr Lanka won.
What is perhaps more revealing about this case though is that in the hearing, virologist and court appointed expert Prof Andreas Podbielski agreed that all six papers inherently assumed the existence of the virus, and none of them showed a virus as a clearly isolated, independent entity with proper controls.
And this type of challenge is being repeated elsewhere. It seems that confidence in the ‘no evidence for viruses’ camp is growing as another similar virus confirmation fund looks for evidence of pathogenic viruses. One established by Tim West on Substack currently stands at £77k and is unclaimed.
Virology tends towards circular citation chains and elusive primary evidence
Sam Bailey has produced a series of resource videos that trace the references, links, and citations used to support claims about various viruses. Her analysis reveals that the evidential foundations of virology are deeply tangled and hard to make sense of.
She highlights circular citation chains — for example, CDC statements that rely on, and refer back to other CDC webpages as evidence, or textbooks that assert viruses as causative agents without presenting primary evidence. She notes how difficult it is to locate original studies that actually establish causation. Where original papers are cited, she shows that they often demonstrate epidemiological patterns rather than causal proof. And where experimental studies are referenced, these frequently rely on tissue-culture systems, lack proper purification, and omit meaningful controls.
Virology has to incorporate the idea that viruses are only intermittently alive
Without periods of biological inertness, viruses would violate core principles of metabolism, thermodynamics, and biological self-maintenance. As a result, the virus hypothesis requires viruses to be biologically active only when embedded within a host cell, and inert outside cells and between hosts.
To a non-virology-trained mind though, this is profoundly counterintuitive: sure, many living systems can become dormant, but this is different, nothing else in biology is thought to alternate between complete metabolic inertness and biological activity. Since this idea of an intermittently ‘alive’ virus has no precedent elsewhere in biology, it begs the question of whether it was introduced to preserve a hypothesis that would otherwise conflict with basic principles of life.
The virus hypothesis gets treated as a fact
By now, I had become proficient at spotting the different kinds of reasoning that the world of virology routinely presents in order to maintain certainty. Drawing on what I could find online, and the discussions with virologits posted by virology researcher Mike Stone, I enlisted AI to help me categorise the 15 main ways virology presents beliefs as scientific fact:
-
Circular reasoning
“The test proves the virus exists, and the virus exists because the test detects it.” -
Model substitution
“The laboratory model behaves like a virus, therefore a virus exists in nature.” -
Comparative theory dismissal
“No alternative explains the patterns as well as viruses do. -
Pragmatic closure / scepticism deflection
“If we treat viruses as hypothetical, science becomes impossible.” -
Non-falsifiability (self-sealing logic)
“If you get sick, the virus caused it; if you don’t, the vaccine worked.”
-
Convergence reification
“Multiple indirect observations, interpreted through the same assumption, are proof that the assumed entity exists.” -
Inference to the best explanation / causal indispensability
“Without viruses, the data make no sense — therefore viruses are real.” -
Predictive success reified as existence
“The model predicts some outcomes well, so the entity must exist.” -
Procedural redefinition of proof
“Science has evolved; direct demonstration is no longer required.” -
Correlation elevated to causation
“This marker appears when illness appears, therefore it must be the cause.”
-
Test reification
“A positive test result means the virus is present, by definition.” -
Missing or assumed controls
“Observed effects can be attributed to the virus even though no independent controls rule out other causes.”
-
Functional definition fallacy
“Whatever produces these effects is, by definition, a virus.” -
Authority substitution / consensus reification
“Viruses are real because institutions, textbooks, and experts agree.” -
Ad hoc rescue clauses
“The virus wasn’t found because it’s latent, asymptomatic, hidden, or below detection limits.”
So what do I say to the curious questioner from our community health session who sparked this enquiry by asking ‘how do we know viruses exist’?
I’ll tell them that I looked everywhere for proof that viruses exist, and I couldn’t find it. No one has ever directly shown a virus to exist as an independent, causative entity, and natural transmission hasn’t been directly demonstrated either. What I found instead was a fragile hypothesis held together by a self-reinforcing system of models, tests, and interventions that all presuppose the thing they claim to prove.
I’ll tell them to check my findings for themselves.
I’ll also share something more personal with them. Exploring this topic was quite disorientating at times, but along the way I noticed that my relationship to my own health quietly changed. I realised that my earlier understanding of illness carried an implicit belief that I was vulnerable to random, invisible attacks from the outside. I realised that this left me feeling powerless, and that I had learned to hand over responsibility for my health to experts, trusting that they would protect me.
What I hadn’t noticed was how a subtle background fear had always accompanied that worldview — until it faded. As my understanding shifted, so did that fear. If health is something that emerges from everyday conditions — how we live, eat, move, rest, and relate — then I no longer need to see myself that way. Health becomes less frightening, less mysterious, and something that feels far more within my own hands.
But I’ll also have to tell them that one doubt remains
After this whole unexpected mind-bending journey of discovery, for me there remains just one whopping doubt about my conclusion that I don’t know how to dismiss. It’s the kind of doubt that just might save virology, and it is this:
It only took me a few days to explore this topic – anyone could do it. Journalists could do it, GPs could do it, virologists could do it.
If it were really true that there’s no evidence for the existence of viruses, and it is this easy to discover, then surely this extraordinary fact would have been front page news long ago.
Our brightest and best health experts would be well aware of all this. Textbooks would have been changed, doctors would have altered the way they care for their patients, students would have rebelled against institutions for abandoning basic scientific standards, governments would have discarded their pandemic policies, and our tax dollars would have been spent elsewhere.
None of this has happened, so it just can’t be true that there is no evidence for viruses – can it?